


New Mexico Medical Board Files Complaint in Woman’s Death From Abortion
3/12/18
Operation Rescue is reporting that a complaint has been filed against a New Mexico abortionist by the state medical board with the intent of investigating a woman’s death from abortion in 2017:
A complaint filed by pro-life activist Tara Shaver of Abortion Free New Mexico has prompted the New Mexico Board of Medicine to initiate a board complaint in order to further investigate abortionist Curtis Boyd, 80, and his conduct during a late-term abortion complication that left Keisha Atkins, 23, dead on February 7, 2017.
In a letter from the New Mexico Medical Board dated March 2, 2018, Shaver was notified that a review by the Board’s Executive Committee determined that Shaver’s allegations warranted “further formal review to determine whether the licensee [Boyd] is in violation of the Medical Practices Act.”
Atkins was at least six months pregnant when she went to Southwest Women’s Options to begin a late-term abortion procedure:
Four days later, on February 3, 2017, Atkins returned to SWO for the completion of the abortion where she displayed labored breathing and signs of sepsis, a systemic, life-threatening infection.
An ambulance was called to transport Atkins from the abortion facility to UNM Medical Center for emergency treatment, but it was later cancelled. Atkins eventually was transported to UNM Medical Center by unknown means where she died hours later.
The autopsy suspiciously claimed Atkins’ pregnancy was the cause of her death, and that her pregnancy resulted in a fatal “pulmonary thromboembolism due to pregnancy.”
However, closer inspection of results within the autopsy report revealed that the patient’s cause of death was more likely attributable to a septic infection caused by repeated insertion and removal of laminaria dilators, along with the fact that she carried her dead baby for four days after Boyd initiated his or her death in the womb on the first day of the abortion procedure. It is also possible that unsanitary conditions or practices contributed to the development of sepsis.
That infection triggered the fatal onset of a clotting disorder called Disseminated Intravascular Coagulation (DIC), which resulted in internal organ hemorrhaging and pulmonary thromboembolism.
Abortion Linked to Higher Death Rates Among Women
Research on death records from three countries — the U.S., Finland and Denmark — have found higher rates of death among women who had abortions compared to women who gave birth.
Further, a recent systematic review that examined 989 studies of deaths associated with pregnancy outcomes found that legal abortion contributes to a fifty percent increased risk of premature death in women.
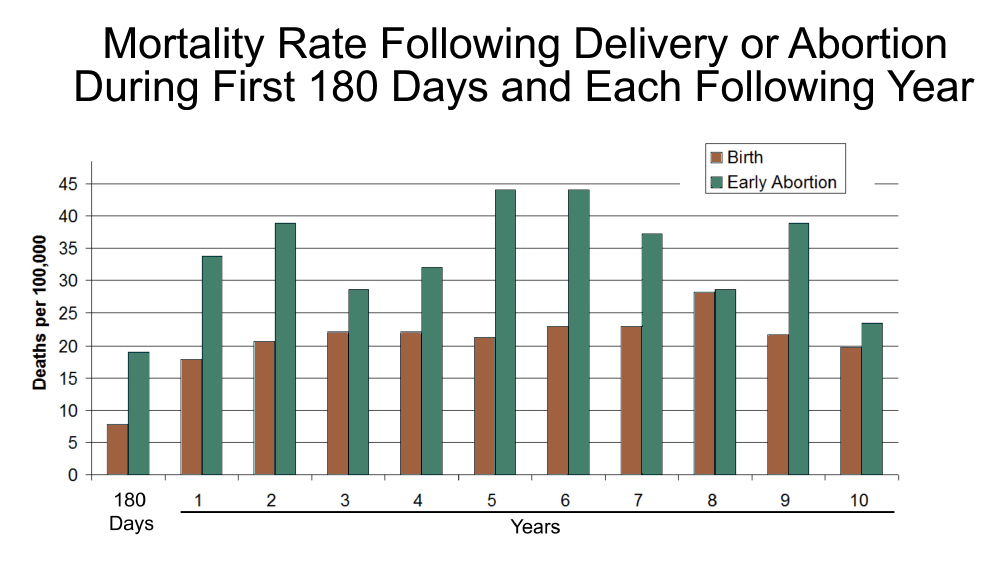
Within the first 180 days, the risk of death from any cause is over twice as high following abortion compared to that following delivery. The risk of early death remains elevated for at least ten years (Figure 1).
Both abortion and miscarriage are linked to elevated mortality rates, but the effect is more strongly associated with induced abortions.
The largest portion of premature deaths following pregnancy loss are due to suicides, accidents, homicides, and some natural causes, such as circulatory disease, which are known to be associated with stress.
The reviewers concluded that these findings are best explained by the psychological effects of pregnancy loss, which contribute to elevated levels of stress, substance abuse, risk taking, and self-destructive behaviors.
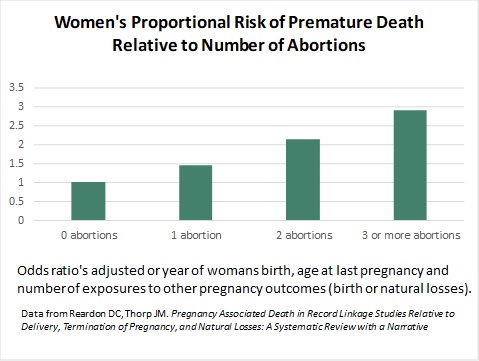
The studies reviewed also reveal a dose effect, with each exposure to abortion adding approximately a 50 percent increased risk of premature death compared to women who have never had abortions (Figure 2).
In contrast, delivering two or more pregnancies improves longevity. Delivery is also linked with a reduction in mortality risks associated with abortion or miscarriage alone.
Women’s Deaths From Abortion Go Unnoticed
While pro-life activists worked to uncover and call attention to the circumstances surrounding Atkin’s death, women’s deaths from abortion are often overlooked and uncounted. As Dr. Lenora Berning has pointed out:
Abortion is one of the most frequently performed surgical procedures in the United States, yet it is the least regulated. It is the only elective surgical procedure that I know of in which the doctor performing the procedure is not responsible for follow-up care, nor does he or she take an active role in dealing with the complications. Not only this, but the very nature of abortion clinics, which practice in isolation from the rest of the medical community, keeps the abortion provider free from accountability for these complications.
Those who support abortion on demand will claim that the reported complication rate for abortions is low. They may be right. Not necessarily because there are few complications, but because the complications are underreported. They are underreported because there is no accurate process in place today to quantify the harmful repercussions of abortion. The abortion industry has successfully kept abortion and abortionists free from the type of review, regulation, and accountability that is an integral part of the rest of the medical profession.
In her statement, Berning went on to cite cases that she had treated involving women who had been injured or killed as a result of mistakes by abortionists. She noted:
Had this quality of care been provided by any other medical provider — family physician, obstetrician, or emergency physician — it would be considered grossly negligent. By an abortion provider, it does not even cause a stir. In fact it goes unnoted and unreported. …
There is no other practice of medicine where people can suffer and die from complications of your intervention without your being in some way professionally accountable, involved in their care, and at the very least, made aware of it — except abortion.
Indeed, many states do not even require abortionists to report complications or injuries from abortion at all:
The U.S. abortion data and reporting system, unlike many other countries, relies completely on voluntary reporting. No federal law requires the reporting of abortion numbers, complications or deaths. (Denmark, in contrast, requires mandatory reporting by providers of all induced abortions.)
In fact, only two national organizations collect abortion data in the United States: the Centers for Disease Control and Prevention, a federal government agency, and the private abortion advocacy group, the Alan Guttmacher Institute. Reporting of abortion data to both is completely voluntary and not all states participate.
Even the most basic statistics about abortion — for example, the annual number in the United States provided by the CDC — is based entirely on estimates, and is therefore vulnerable to human error. How reliable can the annual number of abortions be if California, which used to report approximately one-quarter of all abortions across the nation annually, hasn’t reported its data to the CDC for several years?
It’s impossible to say how safe abortion is in the United States when only 26 states require providers to report injuries and complications from abortion.
~~~
Learn More:
Each Abortion Increases Women’s Risk of Premature Death by 50 Percent, New Study Reports
Higher Death Rates After Abortion Found in U.S., Finland and Denmark: Studies Find Abortion Is Not Safer Than Childbirth
Abortionists Are Not Held Accountable for Mistakes: A Physician Speaks
“Invisible” Abortion Deaths
Why “Accidental Death is the Default Setting for Coroners” When Abortion Is Involved
The Cover-Up: Why US Abortion Mortality Statistics Are Meaningless
Get Help:
Pregnancy Help and Resources
Pregnancy Help Worldwide
Center Against Forced Abortions
Help & Healing After Abortion
Help After Abortion Worldwide