

Abortion Complications And Risk– After Abortion
There are wide variety of complications reported after an abortion. Many are minor. Some are severe. This article is focused on complications affecting physical health.
Emotional and mental health complications are more common than physical complications. These are addressed in a separate article on abortion and mental health.
The Frequency of Physical Complications after an Abortion: 1.3 to 30.5%
How often does abortion involve physical complications?
Answers to that question will vary depending on two factors. First, the timeframe the researcher chooses to examine. The longer the time period examined, the more complications will be discovered.
Second, on the range of complications considered. For example, some researchers may consider only life-threatening complications that occurred within a few days, weeks or months after the abortion. Others will include long-term effects, such as infertility or a general decline in physical health.
The highest rate of complications that has been reported 30.5%. This is the rate reported by women in interviews averaging 10 years after their abortions. In this study, 30.5% of women reported having one or more physical complications they blamed on their abortions.1 This high rate included both immediate and delayed complications. It also included complications some people may consider minor.
By contrast, another study examined only complications requiring emergency room treatment within six weeks of an abortion. By narrowing both the time frame and type of complications considered, this study reported the lowest rate of complications. The authors reported only 5.2% of women sought ER treatment following a medication abortion, 1.3% following a first-trimester surgical abortion, and 1.5% following a late term surgical abortions.2
Between these two extremes, another study tracked any complications treated within 21 days of an abortion, including those treated by a general practitioner or obstetrician. This study found that 10% of women undergoing first trimester surgical abortions experienced at least one complication, with 2% enduring a “major” complication.3
Yet another approach, looking at additional surgical steps, reported abortion complications requiring additional surgical intervention to control bleeding, to remove retained tissue, or to terminate a continuing pregnancy (as in the case of a twin) to occur following 2% to 10% of all abortions.4
A Quick Overview of Physical Complications from Abortion
Minor side-effects may include:
- cramping
- nausea
- headache
- dizziness
- fatigue
During, and immediately after an abortion, the greatest risk is bleeding, or even hemorrhage. Bleeding may result from:
- cervical laceration
- uterine perforation
Rare, but serious complications include:
- blood clots
- embolism
- negative anesthesia reactions
The most common complication is infection. Infection may be caused by:
- lacerations
- perforations
- retained tissue
- unsterile conditions
- an existing infection, such as a venereal disease, that is spread or made worse.
Any of these abortion related infections may contribute to infertility, scarring of the uterus, blockage of the fallopian tubes, or other negative effects on future reproductive health.
Another immediate complication is called an “incomplete abortion.” This means some tissue may be left behind. If it is not removed, it can begin to rot and cause an infection, even a life threatening infection. An incomplete abortion requires a second treatment to remove the dying tissue.
Longer term complications of abortion include elevated risk of:
- premature death
- cervical incompetence
- premature or low birth weight deliveries
- infertility or difficulty becoming pregnant
- lower general health; greater need for medical services
- endometritis
- ectopic pregnancy
- salpingitis or pelvic inflammatory disease (PID)
- placenta previa
- death from cardiovascular diseases
- sleep disorders
- substance abuse
- suicide and other mental health problems
The rates of increased risk for these complications are described further below.
Teenagers are at higher risk of suffering many abortion related complications. This is true of immediate complications, long-term reproductive problems and emotional risks. (See Teen Abortion Risks: A Medical Fact Sheet)
Abortion is Linked to Premature Death
Life expectancy is a good general measure of health. Record linkage studies show that abortion is linked to an increased risk of death compared to non-pregnant women, those who give birth, and even those who have a miscarriage.5 This increased risk of death includes suicide, substance abuse related deaths, and elevated risk of death associated with cardiovascular diseases and some cancers.
The Myth that Abortion is Safer than Childbirth
You will often hear the claim that abortion is much safer than childbirth. But those claims are based on comparisons between the reported number of deaths due to abortion and childbirth.6
What abortion supporters fail to tell you is that there is no standardized process for reporting deaths linked to abortion. In most cases, coroners completing death certificates will have no knowledge of prior abortions. As a result, reliance on death certificates alone has led to very misleading claims about abortion’s safety.7
Accurate comparisons require record linkage: cross checking all death certificates with abortion records.
When this is done, researchers have found that 99% of abortion associated deaths were missed by reliance on death certificates alone.8
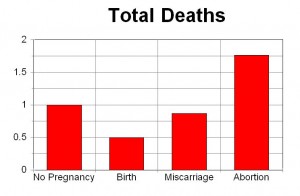
The only way to truly compare death rates between abortion and child birth is through record linkage. When this is done, literally all record linkage studies (from four countries) show that abortion is associated with an increased risk of premature death.5 Premature death following an abortion is more common than following birth, miscarriage, or not being pregnant in the prior year.5
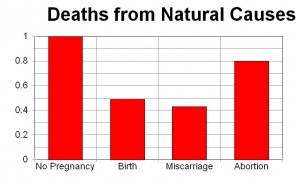
In one of these record linkage studies, women who aborted in the year prior to their deaths were 60 percent more likely to die of natural causes (Figure 2).9 They were also seven times more likely to die of suicide, four times more likely to die of injuries related to accidents, and 14 times more likely to die from homicide compared to women who gave birth.
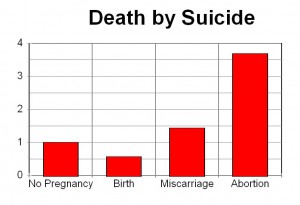
Women who had abortions were 3.4 times more likely to commit suicide compared to women who had not been pregnant in the previous year and 6 times more likely to commit suicide than women who delivered.
Researchers believe the higher rate of deaths related to accidents and homicide may be linked to higher rates of suicidal or risk-taking behavior.5,9,10
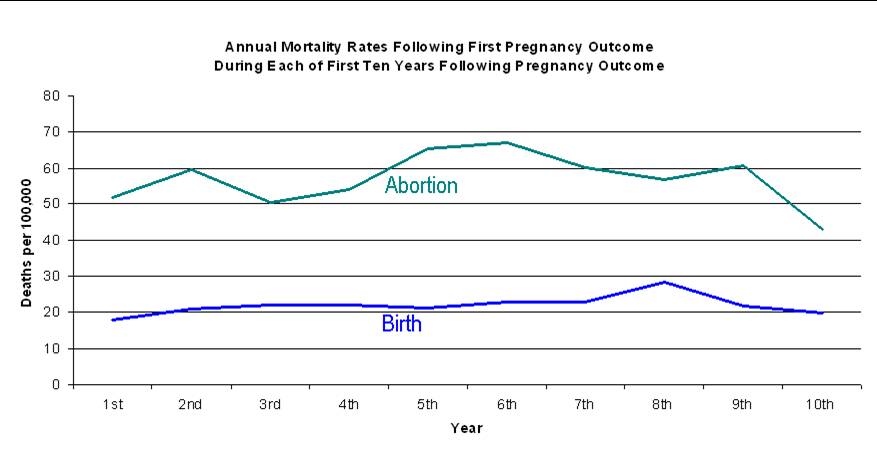
Two studies of the entire population of women in Denmark published in 2012 have shown similar results. The first found that the risk of death following abortion remains higher in each of the first ten years following the abortion (Figure 4).11
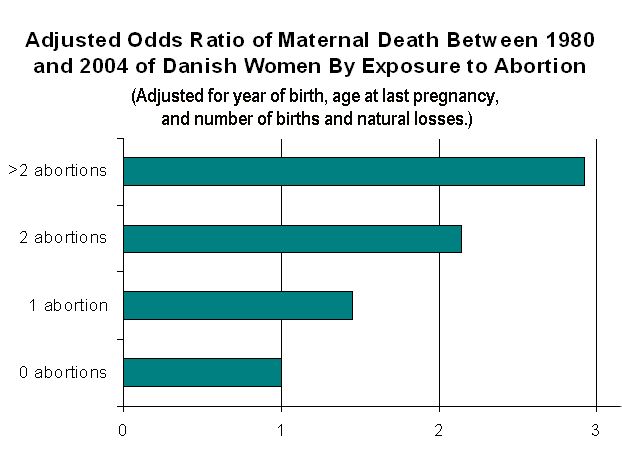
The second found that the risk of death increases with each abortion, 45% after one abortion, 114% after two abortions, and 192 percent after three or more abortions.12 (Figure 5)
{kind=link}
Uterine Perforation
Between 2 and 3% of all abortion patients may suffer perforation of their uterus. This complication injuries will often remain undiagnosed and untreated unless laparoscopic visualization is performed.13–15 The risk of uterine perforation is increased for women who have previously given birth and for those who receive general anesthesia at the time of the abortion.16,17 Uterine damage may result in complications in later pregnancies and may eventually evolve into problems which require a hysterectomy, which itself may result in a number of additional complications and injuries including osteoporosis.
Cervical Lacerations
Significant cervical lacerations requiring sutures occur in at least one percent of first trimester abortions. The risk of cervical damage is greater for teenagers, for second trimester abortions, and when practitioners fail to use laminaria for dilation of the cervix.15,18–22
Lesser lacerations, or micro fractures, which would normally not be treated may also result in long term reproductive damage. Latent post-abortion cervical damage may result in subsequent cervical incompetence, premature delivery, and complications of labor.
Pelvic Inflammatory Disease (PID)
Abortion contributes to the risk of pelvic inflammatory diseases (PID).23–28 PID is a potentially life threatening disease which can lead to an increased risk of ectopic pregnancy, reduced fertility, or infertility.
A chlamydia infection at the time of the abortion increases the risk of PID. In one study, 23% of abortion patients with a chlamydia infection developed PID within 4 weeks.29 Among abortion patients without a chlamydia infection, 5% developed PID within 4 weeks.29
Other infections,such as mycoplasma genitalium or Group B strepococci, are also linked to increased risk of PID following an abortion.30,31
Endometritis
Abortion increases the risk of endometritis.21,32–34 This is true for all, but women, but especially for teenagers, who are 2.5 times more likely acquire endometritis following abortion compared to older women.21
Ectopic Pregnancy
Abortion is significantly related to an increased risk of subsequent ectopic pregnancies. Ectopic pregnancies, in turn, are life threatening and may result in reduced fertility.35,36 The greatest risk of ectopic pregnancy following an abortion appears to be in cases where there was an infection following the abortion.37
Placenta Previa
Abortion increases the risk of placenta previa in later pregnancies38–40 Placenta previa increases the risk of death for both the mother and child and can contribute to fetal malformation and excessive bleeding during labor.
Subsequent Pre-Term Deliveries, Low Birth Weight, and Handicapped Newborns
In subsequent pregnancies, women with a history of abortion are at greater risk of premature delivery and low birth weight children.41–44 Each abortion increases these risks.
Pre-term delivery increases the risk of neonatal death and handicaps such as cerebral palsy.43,45
Increased Risks for Women Seeking Multiple Abortions
In general, most of the studies cited above reflect risk factors for women who undergo a single abortion. These same studies show that women who have multiple abortions face a much greater risk of experiencing these complications. This point is especially noteworthy since approximately 45% of all abortions are for repeat aborters.
Lower General Health
In a survey of 1,428 women researchers found that pregnancy loss, and particularly losses due to induced abortion, was significantly associated with an overall lower health.46 Multiple abortions correlated to an even lower evaluation of “present health.” While miscarriage was also detrimental to health, abortion was found to have a greater correlation to poor health.
The link between abortion and a decline in health is also suggested by studies showing an increase in doctor’s office visits and medication47 and also the elevated risk of death from natural causes.5
Increased Risk for Contributing Health Risk Factors
Abortion is significantly linked to behavioral changes such as self-destructive behaviors, promiscuity, smoking, drug abuse, eating disorders and other mental health issues.10,48
This overlap between multiple factors makes it more difficult to sort out the direct and indirect links between abortion and specific complications. For example, promiscuity and abortion are each linked to increased rates of pelvic inflammatory disease, ectopic pregnancies, and infertility. Which contributes most is unclear. But if promiscuity is itself a reaction to post-abortion trauma, or loss of self-esteem, abortion may be both a direct and indirect cause of such fertility problems.
Cervical, Liver and Breast Cancer
Abortion is linked to higher rates of cervical cancer.49–51 In one study, women with a history of one abortion face a 2.3 times higher risk of having cervical cancer.49 The risk doubles, to 4.92 times higher risk, if a woman has two or more abortions.
Research also indicates that there may be a 60% increased risk of liver cancer after one abortion, and a 110% increased risk after two or more abortions.52
A link between abortion and breast cancer has also been identified in numerous studies.53–55 In one compilation of 36 studies, for example, there was a 44%, 76% and 89% increased risk of breast cancer following one, two, and three abortion, respectively.53 The fact that each abortion increases the risk is called a dose effect. Each dose increases the negative effect. This is a strong indicator that abortion is a direct contributing cause for breast cancer. In the case of breast cancer, it thought that the cancer risk may be due to disruption of the hormonal changes in the breast during pregnancy. At the very least, abortion may disrupt the protective effects of full term pregnancy.
Higher rates of cancer following abortion may also be due to indirect effects. For example, depression and anxiety are linked to elevated risks of cancer.56 This may indicate that higher levels of stress weaken the immune system.
Psychological Abortion Complications
A review of the psychological complications of abortion is at this link.
More Resources
REFERENCES
1. Rue, V. M., Coleman, P. K., Rue, J. J. & Reardon, D. C. Induced abortion and traumatic stress: A preliminary comparison of American and Russian women. Med. Sci. Monit. 10, SR5–SR16 (2004).
2. Upadhyay, U. D. et al. Incidence of Emergency Department Visits and Complications After Abortion. Obstet. Gynecol. 125, 175–183 (2015).
3. Joint study of the Royal College of General Practitioners and the Royal College of Obstetricians and Gynaecologists. Induced abortion operations and their early sequelae. J. R. Coll. Gen. Pract. 35, 175–180 (1985).
4. Kruse, B., Poppema, S., Creinin, M. D. & Paul, M. Management of side effects and complications in medical abortion. Am. J. Obstet. Gynecol. 183, S65–S75 (2000).
5. Reardon, D. C. & Thorp, J. M. Pregnancy associated death in record linkage studies relative to delivery, termination of pregnancy, and natural losses: A systematic review with a narrative synthesis and meta-analysis. SAGE Open Med. 5, 205031211774049 (2017).
6. Reardon, D. C. Rebuttal of Raymond and Grimes on Mortality Comparison of Abortion and Childbirth. Linacre Q. 79, 259–260 (2012).
7. Reardon, D. C., Strahan, T. W., Thorp, J. M. & Shuping, M. W. Deaths associated with abortion compared to childbirth–a review of new and old data and the medical and legal implications. J. Contemp. Health Law Policy 20, 279–327 (2004).
8. Gissler, M., Berg, C., Bouvier-Colle, M.-H. & Buekens, P. Methods for identifying pregnancy-associated deaths: Population-based data from Finland 1987-2000. Paediatr. Perinat. Epidemiol. 18, 448–455 (2004).
9. Gissler, M., Kauppila, R., Meriläinen, J., Toukomaa, H. & Hemminki, E. Pregnancy-associated deaths in Finland 1987-1994–definition problems and benefits of record linkage. Acta Obstet. Gynecol. Scand. 76, 651–657 (1997).
10. Reardon, D. C. The abortion and mental health controversy: A comprehensive literature review of common ground agreements, disagreements, actionable recommendations, and research opportunities. SAGE Open Med. 6, 205031211880762 (2018).
11. Reardon, D. C. & Coleman, P. K. Short and long term mortality rates associated with first pregnancy outcome: population register based study for Denmark 1980-2004. Med. Sci. Monit. 18, PH71-6 (2012).
12. Coleman, P. K., Reardon, D. C. & Calhoun, B. C. Reproductive history patterns and long-term mortality rates: A Danish, population-based record linkage study. Eur. J. Public Health 23, 569–574 (2013).
13. Kaali, S. G., Szigetvari, I. A. & Bartfai, G. S. The frequency and management of uterine perforations during first-trimester abortions. Am. J. Obstet. Gynecol. 161, 406–408 (1989).
14. White, M. K., Ory, H. W. & Goldenberg, L. A. A case control study of uterine perforations documented at laparoscopy. Am. J. Obstet. Gynecol. (1977). doi:10.1016/0002-9378(77)90642-1
15. White, K., Carroll, E. & Grossman, D. Complications from first-trimester aspiration abortion: a systematic review of the literature. Contraception 92, 422–438 (2015).
16. Grimes, D. A., Schulz, K. F. & Cates, W. J. Prevention of Uterine Perforation During Curettage Abortion. JAMA J. Am. Med. Assoc. (1984). doi:10.1001/jama.1984.03340400036021
17. Grimes, D. A., Schulz, K. F., Cates, W. & Tyler, C. W. Local versus general anesthesia: Which is safer for performing suction curettage abortions? Am. J. Obstet. Gynecol. (1979). doi:10.1016/0002-9378(79)90731-2
18. Schulz, K. F., Grimes, D. A. & Cates, W. MEASURES TO PREVENT CERVICAL INJURY DURING SUCTION CURETTAGE ABORTION. Lancet (1983). doi:10.1016/S0140-6736(83)92464-9
19. Castadot, R. G. Pregnancy termination: Techniques, risks, and complications and their management. Fertility and Sterility 45, 5–17 (1986).
20. Cates, W., Schulz, K. F. & Grimes, D. A. The Risks Associated with Teenage Abortion. N. Engl. J. Med. 309, 621–624 (1983).
21. Burkman, R. T., Atienza, M. F. & King, T. M. Morbidity risk among young adolescents undergoing elective abortion. Contraception (1984). doi:10.1016/0010-7824(84)90093-3
22. Montmasson, H., Bertrand, P., Perrotin, F. & El-Hage, W. Facteurs prédictifs de l’état de stress post-traumatique du postpartum chez la primipare. J. Gynécologie Obs. Biol. la Reprod. 41, 553–560 (2012).
23. Lin, T. B. et al. Long-term physical health consequences of abortion in Taiwan, 2000 to 2013 A nationwide retrospective cohort study. Med. (United States) 97, (2018).
24. Westergaard, L., Philipsen, T. & Scheibel, J. Significance of Cervical Chlamydia Trachomatis Infection in Post-abortal Pelvic Inflammatory Disease. Obstet. Gynecol. 60, 322–5 (1982).
25. Chacko, M. R. & Lovchik, J. C. Chlamydia trachomatis infection in sexually active adolescents: prevalence and risk factors. Pediatrics 73, 836–40 (1984).
26. Barbacci, M. B. et al. Postabortal endometritis and isolation of Chlamydia trachomatis. Obstet. Gynecol. 68, 686–90 (1986).
27. Duthie, S. J. et al. Morbidity after termination of pregnancy in first trimester. Genitourin. Med. 63, 182–7 (1987).
28. Sørensen, J. L., Thranov, I., Hoff, G. & Dirach, J. Early- and late-onset pelvic inflammatory disease among women with cervical Chlamydia trachomatis infection at the time of induced abortion – A follow-up study. Infection 22, 242–246 (1994).
29. Radberg, T. Chlamydia Trachomatis in Relation to Infections Following First Trimester Abortions. Acta Obs. Gynoecological (Supp. 93) 54, (1980).
30. Bjartling, C., Osser, S. & Persson, K. The association between Mycoplasma genitalium and pelvic inflammatory disease after termination of pregnancy. BJOG An Int. J. Obstet. Gynaecol. 117, 361–364 (2010).
31. Stray-Pedersen, B. et al. Induced abortion: microbiological screening and medical complications. Infection 19, 305–8
32. Carlsson, I., Breding, K. & Larsson, P. G. Complications related to induced abortion: A combined retrospective and longitudinal follow-up study. BMC Womens. Health 18, (2018).
33. Hamark, B. & Forssman, L. Postabortal endometritis in chlamydia-negative women – Association with preoperative clinical signs of infection. Gynecol. Obstet. Invest. 31, 102–105 (1991).
34. Osser, S. & Persson, K. Postabortal pelvic infection associated with Chlamydia trachomatis and the influence of humoral immunity. Am. J. Obstet. Gynecol. 150, 699–703 (1984).
35. Tharaux-Deneux, C., Bouyer, J., Job-Spira, N., Coste, J. & Spira, A. Risk of ectopic pregnancy and previous induced abortion. Am. J. Public Health 88, 401–405 (1998).
36. Marchbanks, P. A., Annegers, J. F., Coulam, C. B., Strathy, J. H. & Kurland, L. T. Risk factors for ectopic pregnancy. A population-based study. JAMA 259, 1823–7 (1988).
37. Chung, C. S., Smith, R. G., Steinhoff, P. G. & Mi, M. P. Induced abortion and ectopic pregnancy in subsequent pregnancies. Am. J. Epidemiol. 115, 879–87 (1982).
38. Barrett, J. M., Boehm, F. H. & Killam, A. P. Induced abortion: A risk factor for placenta previa. Am. J. Obstet. Gynecol. (1981). doi:10.1016/0002-9378(81)90702-X
39. Ananth, C. V., Smulian, J. C. & Vintzileos, A. M. The effect of placenta previa on neonatal mortality: A population-based study in the United States, 1989 through 1997. Am. J. Obstet. Gynecol. 188, 1299–1304 (2003).
40. Ananth, C. V., Smulian, J. C. & Vintzileos, A. M. The association of placenta previa with history of cesarean delivery and abortion: A metaanalysis. in American Journal of Obstetrics and Gynecology 177, 1071–1078 (Mosby Inc., 1997).
41. McCarthy, F. P. et al. Pregnancy loss managed by cervical dilatation and curettage increases the risk of spontaneous preterm birth. Hum. Reprod. 28, 3197–3206 (2013).
42. Saccone, G., Perriera, L. & Berghella, V. Prior uterine evacuation of pregnancy as independent risk factor for preterm birth: a systematic review and metaanalysis. Am. J. Obstet. Gynecol. 214, 572–591 (2016).
43. Calhoun, B. C., Shadigian, E. & Rooney, B. Cost consequences of induced abortion as an attributable risk for preterm birth and impact on informed consent. J. Reprod. Med. 52, 929–937 (2007).
44. Hardy, G., Benjamin, A. & Abenhaim, H. A. Effect of Induced Abortions on Early Preterm Births and Adverse Perinatal Outcomes. J. Obstet. Gynaecol. Canada 35, 138–143 (2013).
45. Jacobsson, B. et al. Cerebral palsy in preterm infants: a population-based case-control study of antenatal and intrapartal risk factors. Acta Paediatr. 91, 946–951 (2002).
46. Ney, P. G., Fung, T., Wickett, A. R. & Beaman-Dodd, C. The effects of pregnancy loss on women’s health. Soc. Sci. Med. 38, 1193–1200 (1994).
47. Berkeley, D., Humphreys, P. C. & Davidson, D. Demands made on general practice by women before and after an abortion. J. R. Coll. Gen. Pract. 34, 310–315 (1984).
48. Burke, T. & Reardon, D. C. Forbidden Grief: The Unspoken Pain of Abortion. (Acorn Books, 2007).
49. Le, M. G., Bachelot, A., Doyen, F. & Kramar, A. [A study on the association between the use of oral contraception and cancer of the breast or cervix: preliminary findings of a French study]. Contracept. Fertil. Sex. (Paris). 13, 553–558 (1985).
50. Pair Dong Wang & Lin, R. S. Induced abortion in Taiwan. J. R. Soc. Health 115, 100–108 (1995).
51. Remennick, L. I. Induced abortion as cancer risk factor: A review of epidemiological evidence. Journal of Epidemiology and Community Health 44, 259–264 (1990).
52. La Vecchia, C., Negri, E., Franceschi, S. & D’Avanzo, B. Reproductive factors and the risk of hepatocellular carcinoma in women. Int. J. Cancer 52, 351–354 (1992).
53. Huang, Y. et al. A meta-analysis of the association between induced abortion and breast cancer risk among Chinese females. Cancer Causes Control 25, 227–36 (2014).
54. Brewster, D. H., Stockton, D. L., Dobbie, R., Bull, D. & Beral, V. Risk of breast cancer after miscarriage or induced abortion: A Scottish record linkage case-control study. J. Epidemiol. Community Health 59, 283–287 (2005).
55. Brind, J., Chinchilli, V. M., Severs, W. B. & Summy-Long, J. Induced abortion as an independent risk factor for breast cancer: a comprehensive review and meta-analysis. J. Epidemiol. Community Health 50, 481–96 (1996).
56. Pan, A., Sun, Q., Okereke, O. I., Rexrode, K. M. & Hu, F. B. Depression and risk of stroke morbidity and mortality: a meta-analysis and systematic review. JAMA 306, 1241–9 (2011).
My health has declined drastically since my abortion. J never linked it to possible implications of the abortion. My menstruation and my hormones are completely out of whack which intuitively thought could be because of the awful decision made…. at the end of the day maybe I deserve to be sick and have womanly problems
Where can I get the information such as who wrote this article and when it was published to use it as a reference for a paper?
Hi Kirsten, this is an ongoing page that has been updated over time, with new information added as new studies are published. So there is no single author — and no publication date as we keep putting new stuff on the page. If you want to find a source about a particular study you should check the citations at the bottom of the page. You can also click on the research link above to see links to articles on individual studies.
I want more about why no menstruation after an abortion then???
Generally, menstruation should resume after an abortion. If it does not, you should see a physician.
Generally abortion takes place in villages. When women are pregnant if girl is inside her womb then her husband pressures for abortion. Then it is bad for whole mankind because if girls are killed day by day how can our country be developed. In villages many people’s thoughts are that boys are breadwinners while girls are burden for them.
2 years a go i had also used medication to avoid pregnacy due to my personal problem.later on i did not have regular period only begins 4-5 months if it begins then also bleed 1 2 months .then i went to doctor and investigation shows that usg-pcod.then doctor oder to take oral bith control pills for three months .i start to took it when i took tha my preiod was regular then again when i stop same last for 2months again i went again he suggest to take the same now i m not taking pills.and having same problem.plz tell me what i should do ?
Hello Kabita,
Sorry you are having problems about this. Unfortunately, we can’t diagnose medical problems or give that kind of advice. You need to talk with your doctor or even get a second opinion from another doctor. Maybe that would be a good idea if you feel like your problems are not being addressed. If you are in the U.S., you can contact the American Association of Pro-Life Ob/Gyns as perhaps they can put you in touch with someone who can help.
Wait what does the baby feel during an abortion because I heard if you do it late the baby well feel the abortion. Is that true.
Here are some links to articles and information on fetal pain:
What Science Reveals about Fetal Pain http://www.frc.org/fetalpain
Unborn babies can feel pain http://www.nature.com/pr/journal/v70/n5s/full/pr2011378a.html
Doctors on Fetal Pain web site http://www.doctorsonfetalpain.com/
Here’s a study that recommends that anesthesia be given to unborn children after the middle of pregnancy during surgery, because anesthesia given to the mother might not be enough:
http://www.nature.com/pr/journal/v70/n5s/full/pr2011378a.html
I’m not sure if you are asking just for information or if you or someone you know is facing the possibility of abortion. If that’s the case, you need to have all the facts and information about the options before making a decision. There are people out there who can help you through this. You can contact Option Line for free, confidential 24-hour help, or visit here for a list of organizations that can provide free resources, counseling and support. (From outside the U.S., you can email us at elliotinstitute@gmail.com for help in finding a local group).
If you or someone you know is being pressured or coerced to abort, this is wrong and there is help available. You can contact the Center Against Forced Abortions and also go here for more information.
I don’t recommend anyone undergoing such procedures unless it is the absolute only choice you have. I was forced to get an abortion at the age of 16, at age 20 and 21 i gave birth. I got pregnant on three occasions since then and terminated them all. I was feeling like i could barley take care of the two i had and with the sickness i couldn’t take it. Now IN 2015 i had 2 miscarries one in January and one in December. I even heard my babies heartbeat and the next day i was miscarrying. Not to mention the pain,regret,and hurt i feel for all of the babies. Maybe someone can learn from my mistakes, Birth control is the responsible thing to do if you are not prepared for parenthood. I wish i made better decions now i cant give my husband a baby and it hurts him too.
It sounds like a post-abortion healing program may help you to deal with any feelings of loss, grief, or regret that continue to be with you. Please check out our page on tips for finding a post-abortion healing program. Most are free, or available for a very low cost.
i had an abortion early this year and i’ve never been the same… i Felt tha my boyfriend didnt go through what im still going through and i blamed him in such a way that it led to our break-up… how do i heal!!???
Hello, I’m so sorry for what you are going through. Have you seen the healing page at https://afterabortion.org/help-healing ? It has lots of information on finding healing, contacting a support group, what to expect, etc. Healing can be hard to do on your own so I would suggest you contact an organization that can help you. There are lots of groups out there that offer free and confidential support and can walk with you through the healing process, or simply provide a listening ear if you need to talk with someone. I would really encourage you to start there. There is a list of post-abortion healing groups at the end of the healing page. Or, if you are outside of the U.S., you can email me at elliotinstitute@gmail.com and I’ll try to find a group in your area.
thnk u so much for ur help. my husband said if i wud fall pregnant now he wud leave me n th kids….go n start over else where. hes almost the only family i have. am scared tht i might lose him for real at th same time my health is at risk…
i wish to know about pap- smear.
I understand your fear and how isolated you feel if you don’t have close family or friends to rely on. That’s why I strongly encourage you to reach out to one of the help centers I gave links to in my last email. They give not only help, but friendship, and usually from other women who have been through very similar troubles and know how much the friendship of a new friend who understands you can be.
Don’t remain alone in your trials. Everyone needs friends and support from more than one person . . . especially if that person is threatening to leave you if you don’t do everything he wants. I want the best for you . . . and him. And you both need support from others, and likely some marriage counseling so that he can better learn to understand and respect and value your needs. Please call one of the numbers I gave you so that you can get some support from a trained counselor. You are in my prayers.
i have 2 baby boys n dnt wnt a baby yet, i felt pregnant this year and my husband didnt want to have another baby… i had an abortion n soon after i came from the hospital i fell pregnant again, n had another abortion. my husband doesnt want to use a condom n doesnt want me to use contraceptives. i dnt know wat to do coz i feel like am pregnant even now. i have no complications n have no pains but am worried now. please help me
Faith, you are in my prayers. Please know that even if you are unaware of any complications, repeat abortions are very bad for you both physically and emotionally. The hidden effects add up and may erupt ten years down the road.
I strongly encourage you to reach out to a post-abortion support group by checking out our healing resources page. They can put you in touch with a family counselor who can help you and your husband come to a better understanding of each others needs, and the needs of your children.
Your husbands attitude is very confusing. Is he using repeat abortions to punish you . . . or himself . . . for some real or imagined offense in the past?
If you are pregnant again, please check out our resource list for pregnancy help centers. Again, they can help you get family counseling to get to the root of your problems.
If you are pregnant, I understand that the timing to have another baby is not as good as you think it should be. But I also ask you to consider that God may be using this timing as a way to intervene with a gift of life that will also help you and your husband finally address the deeper issues that are between you and have been cycling you through this pattern of repeat abortions. It needs to stop. If you are pregnant, giving birth to this child is a key stop to breaking that cycle.
You are in my prayers.
I want more information about the abortion
What are things that should nd shouldnt happen durring original due date if had Terminated
If you have concerns about physical health after an abortion, I would talk with a doctor and let him or her know the situation. You can also contact the American Assoication of Pro-Life Ob/Gyns at http://www.aaplog.org/aaplog-physician-directory/.
If you are looking for more general information on abortion complications, you can search our research page (https://afterabortion.org/1999/more-research-on-post-abortion-issues/). You can also find more information on research studies at http://www.abortionrisks.org.
I had an abortion and ever since have not felt right, been hospitalized, missed a lot of work and after bothering doctors for weeks finally found out I have liver issues. My symptoms were extreme weakness, lightheaded ness, weight loss, diarrhea, fatigue, incomplete abortion, infection, changes in mood, pain in uterus, low blood pressure, yellowing of eyes, my legs are very weak, divided or torn uterus, black blood, nausea…. The list goes on and on. I need help and answers! The last sonogram showed particles left behind! My doctor told me to return to work! I’m on my feet all day, can a doctor please tell me what is going on??? Or anyone??
We don’t have any doctors on staff who can advise you. If you’re not satisfied with your regular doctor’s recommendation, please seek a second opinion from another physician in your are.
I had an abortion at age 26. Not knowing I was pregnant I had underwent a biopsy for abnormal cells on my cervix, as well as a treatment for chlamydia. I started to feel ill after and cramping, I also had constant nose bleeds and fainted a few times. I then found out I was pregnant and discussed the pregnancy with my husband.
He was very much against me having the baby. Our relationship was doing badly, because at the same time I had also found out that he had cheated on me and given me chlamydia. I was planning to separate and leave the country to go back home and raise the baby as a single mother. But during the next check up no heart beat could be found. I waited until I was 9 weeks along and still there was no heart beat anymore.
Doctors gave me a pill to undergo medical abortion. When I got home I hesitated taking the second pill and my husband began to argue with me. So I placed it in my mouth and held it there for a while before I swallowed it. I then got scared and made myself throw up on the ground, while my husband was yelling at me, saying that I was wasting “600 dollars”. I was bleeding and cramping horribly for weeks.
At the next check up I was not pregnant anymore. I separated from my husband, but shortly after the abortion my health began to deteriorate. It happened so fast I was in utter shock. I don’t know if it is all related to the abortion, but I was healthy before this aside from the HPV. My hair began to fall out and unlike after delivery…it would not stop. An endocrinologist found out that I had a pituitary tumor and raised prolactin levels. My body was producing prolactin for the baby I was meant to nurse. All this made me very sad. It was also found out that I had hypothyroidism and my abnormal cervical cells had turned into cervical cancer. I had to have a LEEP, to burn off affected tissue on my cervix.
When I got the diagnosis, I was in a new relationship, with a man that wanted to have children with me in the future. When I got pregnant, doctors were very worried about my pregnancy because of all my conditions and the LEEP. Some friends and family even advised me to consider abortion because they were worried about my health. I was positive things would be fine and my pregnancy actually went really well. I became healthier and I was glowing. I was the only pregnant woman that could walk two hours to get from A-B while 40 weeks pregnant. My son was developing well and my medical issues were controlled. 1 1/2 months before the due date, I got off the pills I was taking for the pituitary tumor, so I would be able to breastfeed and decided to only have my prolactin monitored. I never went into labor though, or had my water break and my son was delivered via Emergency C-Section at 42 1/2 weeks (doctors had my due date wrong).
I still wonder why I wasn’t able to deliver naturally. After pregnancy, my health issues subsided. My prolactin was stable and while breastfeeding, the pituitary tumor shrank, when my son was a year old my cervical cancer was gone all together with the HPV (it was still there after delivery ). 1 1/2 years after delivery and still breastfeeding, my thyroid was healed…”Hashimoto’s” is usually said to be permanent…well, not for me. The only problem that hasn’t changed is the hair loss. My hair falls out for no reason to the point where it is thin, and then grows back. I don’t know what is causing it at the moment.
My son is almost three and I continue to breastfeed him because I only want the best for him. He is the most important person in my life and I know most mothers would feel like that, would they only let the pregnancy allow to take its course.
Women who have abortions do not know what they are missing out on. I am honestly very tired of the “right to choose” slogan…making it seem as if it is only about the right to decide over your body. Imho you have the right to use birth control, if that fails the Plan B pill….Many “unwanted” pregnancies happen because two people are careless and think that nothing will happen. Such cases make me very sad, it doesn’t have to happen if they take precaution. I am not Christian btw., because I know some argue all Pro Lifers are fanatic Christians. I don’t believe in anything related to Religion. – M. from Germany
my question is what are the main symptons of health risk after abortion. i myself dont believe in killing what the man above have blessed the person with but i cant stop her from doing what has her mind set on. im afraid that i can lose my girlfriend to abortion complications…. am i blowing this out of porpotion and have nothing to worry about or should i be concerned…. i just wish she would change her mind and have this baby and have faith that everything will be ok…. someone please give me feedback… thank you
While there are many physical risks associated with abortion, the psychological risks are more common and can contribute to physical problems, such as lower general health, since psychological stress is hard on the body.
You are not blowing your concerns out of proportion . . . but there is only so much you can do. It sounds like you are doing your best to encourage her to have faith that things will work out. I’d suggest asking her to review the risk factors for psychological problems after an abortion. Hopefully, doing so will get her to better understand that this won’t be as easy to forget as she imagines it to be.
You are all in our prayers.
I always read about how pro-choice means you care about Womens rights and how they feel. However, they never talk about how traumatizing it could be to a Woman who goes through the process.
When my wife first got pregnant I was so scared. I didn’t know how I could afford the baby. We had just started going out. I kept thinking about my finances and how we could survive.
The day my son was born was one of the greatest days of my life. Every day I look at him I am reminded of how lucky I am. I would give up my house and all my possessions if it meant having him by my side.
Now think for a moment. I am just the father. Imagine how my wife feels? She carried him for 9 months. She went through the pain of delivery and the morning sickness. The sleepless nights and worry. She went through so much and she loves her boy more than anyone could.
Yes it’s hard raising kids. It changes your life plan. It puts a stop to some of your plans. It is also the best and most rewarding thing in life.
Then you might say to me, “You don’t know my situation!” You are right. I don’t. But I do know that if you love your child no obstacle will get in the way of you providing for that child.
Then you say, “It’s my body and I can choose to do what I will.” Sorry, you are not talking about your body. You are talking about aborting a baby’s body. You have no right over a baby’s life. Plain and simple.
We talk about education, then why not educate Women about the risks and trauma associated with abortion. I mean warning labels on food are more informative than Planned Parenthood speaking about risks with abortion. Planned Parenthood site talks about possible risks with the procedure, but says overall its safe. No mention about mental trauma.
I am 18years of age and had my abortion in April. After the abortion I was fine because they had to numb me extra cause I was sensitive to the in clinc abortion. Once I got home and the numbing started going away, I started feeling this ripping feeling located where my uterus is, and I only spotted a little blood and brown which I assumed it was just the uterus lining doing what it does when your on your period, the cycle. I never wanted to go back. & even if I did I didn’t have the money, and my Doctor wouldn’t help me because he told me I should follow up with them. They put me on Sprintec Birth Control, because I didn’t know what I wanted to choose. She asked if I wanted the doctor to Choose I said sure. Why when I started my 3month birth control it was fine at first, I actual like my birth control, I have had no side effects like the last birth control I was on. Anyways two months later I been bleeding way before my period [3 weeks before the white pills]. & it has never happened like this before. & I am in pain the ripping feeling again, I’m scared to go to the Hospital I have no insurance an I don’t know what’s wrong. I never mentioned before the abortion I have HPV, ab-normal cells in my ovaries, That’s what my Doctor told me. I don’t know if that mattered. & when I got a pap’s 3 weeks after abortion, it hurt and she asked has it always hurt. Which I have always been sensitive so I said yes and she never said anything. That was that. I am really worried and I don’t know if you have had women before me with the same problem to tell me what I can do to treat it or what might be wrong, I’m also kind of scared to know. I don’t ever want another male doctor down there. It wasn’t his fault, he was only doing his Job, which he has been doing for many of years.
I strongly encourage you to call a post-abortion healing center. You can get help and advise from women who have been in your situation. Even your fear of seeing another doctor about the abnormal bleeding is a sign of how you have been traumatized both psychologically and physically. Don’t let your fear keep you from getting good advise. Most post-abortion healing programs are free or will waive any fees if you can’t afford it. You are in my prayers.
Science recognizes that human life begins at conception. You were once a fertilized egg. If anyone had extinguished your life at any time between that stage and birth, you would not exist today. You did nothing wrong during that time because you were incapable of wrongdoing – so you were an innocent human life. To deliberately extinguish innocent human life is murder. We have murdered in excess of 50 million unborn humans in the USA since the legalization of abortion on demand. The total number of human lives lost during all the years of WW II (all theaters and all causes) is estimated to be 50-70 million. In the USA, murder by abortion is now as common as worldwide deaths during WW II. What is the price we will have to pay for this slaughter?
If babies in utero are incapable of wrongdoing, as you say (which of course they are!) then why do some religious sectors cleanse babies of a so-called ‘Original Sin’? I’m not trying to offend anyone by asking this, I am literally just wondering!
I suggest you look up the difference between “actual sin” and “original sin.” In Christian theology, actual sin includes any willful thought, desire, word, action, or omission that separates us from God’s will. Culpability for actual sin is lessened by obstructions of free will (being coerced or intoxicated, for example) and by ignorance (not knowing the consequences, for example). So while an act may involve very serious sin, guilt may be lessened by defects in will and knowledge.
Babies are free of actual sin, obviously, because they have limited ability and opportunity to willfully act with knowledge in any way that offends God.
Original sin, by contrast, refers to humankind’s origins (root word for “original). God made us to be perfectly able to conform to His holy will. But when Adam and Eve set their wills up against God’s will, choosing to know/define good and evil according to their own minds and wills, this changed the relationship between God and humankind for all generations. This “original sin” means we start out life already broken and separated from the relationship God intended for us when he first created humankind.
Christians believe Jesus came into the world to not only bring mercy and forgiveness for our actual sins, but to also fix at least one consequence of original sin, namely restoring our relationship with God as His children. One way this is done is through baptism, being reborn into the family of God. But other effects of original sin still remain, including a level of conflict and brokenness in our wills and intellects which lead us to continue to struggle with temptations and commit actual sins–often choosing to do that which we know (on some level) we shouldn’t.
check their references…they’re all from the seventies or eighties lol…if you want to be taken seriously at least be relevant 🙂 nice try though
Erica, this is an old post from 1999, so naturally the references are old ones. You will find plenty of current studies listed on our news (https://afterabortion.org/?p=2507) and research pages (https://afterabortion.org/?p=2211), as well as at http://www.abortionrisks.org.
I love your work and i’m willing to join you to help others please
To help, first join our email list so you can stay up to date.
Second, if you are able to help us financially, that would be a huge blessing. Our costs are outrunning expenses.
Third, you might look over our outreach materials and see if there is anything there that you can distribute through your church, work, or some other way.
What is the nursing management in order of priority for woman who undergone induced abortion?
I’m afraid we don’t know. I’m doubtful there even is a standard, but would love to hear about it if you find one . . . or help to develop one.
how can i get an APA reference for this article?
How come this site:
http://www.cancer.gov/cancertopics/factsheet/Risk/abortion-miscarriage
says that according to recent studies done that there is no valid relation between abortions and cancer???
The web page you reference only addresses the breast cancer risk associated with abortion.
This link is to studies showing abortion is associated with a number of cancers.
Regarding the abortion breast cancer link, as you know the whole abortion issue is highly politicized. There was a lot of pressure both within and outside the national cancer institute to explain away and ignore studies showing a link between abortion and breast cancer. If you read their statements and conclusions carefully, it is evident that they admit that studies have found statistically significant associations between abortion and breast cancer, especially for certain subgroups of women, like those with a family history of breast cancer who abort before age 18. But they then go on to argue that this evidence is not sufficiently convincing to warrant “scaring” the public, and there are methodological issues that can be raised to cast doubts on these findings, blah blah blah.
In other words, while in nearly every other case of evaluating medical treatments, evidence of a statistical association is sufficient to raise concerns. Proof that the treatment in and of itself causes the suspected complication is not required before they start warning that the complication MAY be associated with the treatment.
But in the case of abortion, this standard of “warn when in doubt” has been replaced with “innocent until proven guilty by incontestable evidence of a direct, strong causal relationship.” Put another way, the standard of proof has been shifted to such a high bar that the evidence showing statistical associations between abortion and breast cancer can be re-evaluated as not sufficiently convincing to warrant disturbing the peace of mind of women who “need” abortions.
It’s a very paternalistic attitude. Even more importantly, this suppression of risk information is largely driven by the government’s public policy that seeks to reduce birth rates among the poor (which is why so much funding goes into birth control and abortion services around the world, way out of proportion to other health care services). Toward that end, suppressing information about the risks associated with abortion (by raising the standard of proof to one that does not apply to any other medical procedure) serves the “public good” by reducing the chances that poor women will choose against abortion because they are afraid of the physical or psychological consequences. The “abortion is safer than childbirth” argument has proven to be very effective in reassuring women and their families that abortion is “safe and easy.”
It is not safe at all. It has to many risks!
As much as you like to call is that, we are not pro-abortion. No one is pro-abortion. We are pro-choice. Pro-abortion would be if we wanted everyone to have abortions. All the time. No more babies, only abortions. I promote abortion to all pregnant women. I have them sometimes when I’m not even pregnant I’m so pro-abortion! It is pro-choice. I believe in a womans right to chose an abortion if it is right for her, or not have an abortion if it is wrong for her. And we pro-choice women are not stupid. I know what being pregnant means. I know it is a fetus.
Most people who favor legal abortion are pro-choice, like yourself. I can believe that you have no prejudice against women who would rather have their babies than have an abortion.
But there are also many who are truly pro-abortion in that they want on women — especially women of color or women who are poor or less intelligent or “unfit” — to have abortions even if requires deceiving them or pressuring them into consenting to abortion they would otherwise refuse. Other pro-abortionists are dedicated to reducing the world’s population for environmental purposes. Margaret Sanger’s Planned Parenthood was setup and funded precisely for the purpose of reducing birth rates among the “unfit.”
The racist attitudes of some abortion providers was well articulated by Dr. Edward Allred, owner of the largest chain of abortion clinics in California who sees abortion as a means of social engineering. In an interview in The Sand Diego Unino, Allred said:
In short, while everyone who favors “abortion rights” wants to cloak their views in pro-choice, pro-woman rhetoric, there are a great many people who see abortion as a social engineering tool which can be used to control the quantity and quality of people born into the world . . . not for the benefit of each individual woman’s informed choice, but for the benefit of eugenic social policy.
Here’s a quick way to tell the difference.
Ask people who say they are “pro-choice” if they oppose the one child policy in China which includes forced abortion? Hardly a pro-choice policy, is it? If they do, then they are truly pro-choice, because they believe women should be allowed to have or not have children as they choose. But if they defend the right of the state to deny women the right to have children, and to punish them or coerce them into having abortions in order to achieve the goals of the state, then they are not pro-choice. Perhaps you still object to them being called “pro-abortion,” but what label would you prefer for persons who have no objections to women being pressured into unwanted abortions?
I know that there are good people who are pro-choice and not good people who are pro-choice. Just as there are on the anti-choice side. The cases of eugenics you refer to are real, and have happened. Largly back in the 50’s and 60’s, not so much these days with all of the publicity and education that has been done onthe the subject. (though I find it noteworthy that many anti-abortion folks are also anti social programs to help all these woman who may decide to have their children in less than healthy situations, and it seems lately they are also anti-birthcontrol) But I digress. The aweful people you have quoted are aweful people. To me that says the focus should be on education those people, and taking them out of positions of power. I don’t see the answer being taking away the legal medical option for terminating a pregnancy because some scumbags are trying to use it for eugenics. It seems like walking in a wide circle around the problem to stop in in the wrong place, with the wrong person. You want to pull woman out of the river instead of stopping that guy from throwing them in. I am for educating women. We know it is a fetus in there. We don’t need to be told that. But if you want to educate women about how horrible the procedure is, you should also have to educate them about the realities of having a unwanted child, raising them in poverty or as a single mother or the many other consequenses of having a child when you are not ready or willing to do it. Show a video of the procedure. But also show video of women and children living in homeless shelters, trying to eat for a month on foodstamps, the reality of where your life changes from being a college student with a future to dropping out to raise a child. A childs life continues well beyond the pregnancy that doesn’t end in abortion. Be realistic about that too. It isn’t always pretty. It isn’t always fine. A woman isn’t always going to be able to handle it (or she wouldn’t have been considering abortion in the first place.) Women who are pro-choice aren’t always the slutty girls who are having multiples as their method of birth control. Sometimes they are drug addicts, or in their senior year of med school, or already have as many kids at home as they can care for responsibly. In a perfect world maybe they would choose adoption instead. But as a 2X birthmother I can tell you it was hell, I lost my entire family and the child I had later and kept I had to raise with no aunts and uncles, no grandparents because they were all angry about the kids I had “passed off like free samples”. It has been 20 years and I still feel the trauma of having been a 16 year old girl birthing in an empty hospital room. It isn’t always simple and it can’t always be done in the way that is neatest or prettiest for the rest of us to see. It is always a tough choice to make. It is never taken lightly. And it isn’t as easy as just skipping that appointment at the clinic. There are consequences for the woman, and the child forever. They don’t skip off into the sunset with their perfect pretty baby laughing at the lovely surprise life has given them. So if you want fewer abortions (and so do I) we need to first address why women choose them, why women feel that they need them and be helpful in solving those problems too. Not just taking away the abortion. Take away the need for them.
Except, for all of the inconvenient things listed above, there is the option to give the baby up for adoption. That same, poor woman with probably little access to good quality healthcare would NOT be in a better position if she becomes suicidal or if she develops cancer or some other complications. This is a VERY risky procedure, and the poorest, most disadvantaged women are always the least informed — she may develop a post-abortion infection and not even be able to go to the clinic, or know that she should/has the right to free medical care.
Reading your story, I am really sorry that you had to go through the challenge of raising your children all alone – we know that it is very difficult to be a single Mom and I think we all respect you for your decision to keep the children.
However, no one is suggesting that single mothers should not be helped – in fact, e.g. in the US I think pro-life activists are pushing for a mandatory statement of who the father is (checked with DNA testing) and making the father pay alimony if the woman decides to keep the baby.
Other measures to help mothers are also being proposed throughout the world, also for facilitating adoption and cutting the red tape and other useless, inconvenient factors that impede it; the need to help mothers is definitely recognized by pro-lifers.
I used to think it was moral to be pro-choice, too, even though personally, I would NEVER have an abortion myself.
The argument that got to me was not poverty – that I thought would be tough but bearable, and I come from a country that has for a long time been considered “poor(er)” so we’re used to that around here.
No, I honestly thought, making abortion legal would prevent the tragic deaths of many desperate women who would have an abortion anyway, even if it was illegal, under God knows what circumstances/ conditions. But then I looked into the statistics and I realized, that if you acknowledge the unborn baby is a person who has the right to live, then when you crunch down the numbers, then we avoided the deaths of a handful of self-destructing women at the cost of genocide. In my country, the abortion death toll has surpassed 20 million babies — all while women who abort continue to be castrated due to various complications, experience higher rates of suicide, and even sometimes die right on the surgery table — because, while illegal abortion *is* arguably more dangerous than legal abortion, more women abort since it’s legal, the procedure is VERY risky in itself and illegal abortions still happen (especially for teens, who generally have less money and less life experience and can be more emotionally unstable than their mature peers)!
So it does not benefit the mother to have an abortion, and it definitely kills the child. It’s a lose-lose situation.
And the eugenics, that you state only happened in the 50’s and 60’s… Well, it does seem like sci-fi to believe it is still brooding nowadays, isn’t it?
But it’s not sci-fi. Already, thousands of babies are being aborted based on the triple test, because they are *(merely) suspected* of having Down Syndrome. One in 200 women loses a baby (whose odds are stacked up for him/her that s/he is actually perfectly healthy) due to the fact that the amnio done to check the triple test results is a risky procedure. A lot of parents are so engrossed that the child may be “retarded”, and they are so misinformed about the (in)accuracy of this test, that they do not even have the amnio, they just abort directly based on the triple test results.
Pro-choice activists push the agenda that it is a relief to abort such a baby, because what life would it have, and it’s not even euthanasia because “we have to understand (??)” the fetus is but a clump of cells.
And this is the crunch — when all other arguments fail, pro-choice activists will come to you and say, well, it’s not really a baby. It’s not really a person. It has no self-awareness, no moral right to live (until expelled from the womb).
But when you take this criterion, of “self-awareness”, as defining the right to live, the womb may no longer be the final frontier. You can push it to deprive, say, 1 year olds of the “moral right to live”, as is currently being proposed:
http://www.telegraph.co.uk/health/healthnews/9113394/Killing-babies-no-different-from-abortion-experts-say.html
And guess what… The people who are currently in power worldwide? Do you know what the buzzword is in their world?
Overpopulation!
Tough solutions may be required in order to prevent the human race from spiraling out of control. After all, we are soooo hurting the planet. The unworthiest species. A cancer on earth. (Any of these currents of thought sound familiar?)
I think if the pro-abortion groups ever saw an abortion and how that child struggles to avoid the piercing probe that eventually punctures and kills him/her….unless they are true monsters …which some abortion leaders are…the vast majority would reconsider. I guarantee you that as long as mills like Planned Parenthood exist young women will never realize their mistake of this life changing event….until its too late. The usual answer a pro abortion zealot responds with is….”its a woman’s choice…I don’t want to hear what happens…stop describing it!”
Does abortion increase a woman’s chance of getting breast cancer??
It is very well established that the younger a woman is when she carries a baby to full term, the lower her life time risk of breast cancer. In other words, pregnancy is good for a woman’s health and reduces her risk of breast cancer (and many other health problems). So at the very least, having an abortion causes one to lose the benefits which would otherwise occur from giving birth sooner rather than later.
The big question is whether abortion causes an additional risk of breast cancer. Numerous studies have found an independent association between abortion and breast cancer. A meta-analysis (a type of study combining the results of these studies) by Dr. Joel Brind revealed a statistically significant association and Brind. He has proposed that the physical mechanism is caused by the sudden change in pregnancy hormones caused by abortion which unnaturally disrupt changes in the breast tissue which are taking place in early pregnancy. Because of the political controversy over these findings, a committee of experts issued a statement stating their belief that the results of these studies are not sufficiently convincing to warrant public alarm. Joel Brind published a minority opinion that is available online, along with other fact sheets, at Breast Cancer Prevention Institute. You can also find a synopsis of various studies examining abortion and breast cancer at AbortionRisks.org.
Yes and it also causes other types of cancer
Brandon, the article is just a list of risks involved when an abortion is being considered. It is not arguing Pro-Choice or Pro-Life, it is simply stating informational facts about abortions. It is simply giving info, not argument.
You do not mention anything about arguments with what many people argue pro abortion or pro life and if things may become more ugly and you are not very specific about what happens after a abortion
I ve doubt n im confused can any1 help me… I was pregnant n tat s abortion due to some problem. Suppose im again pregnant means that old abortion will be known by doctor a???
I don’t know if your doctor will know about a previous abortion unless you tell him or her. It probably depends on what records the doctor has access too and if it is in those records. That being said, you should let the doctor know your complete medical history, including an abortion. That way if there are any risks or problems that crop up during your pregnancy the doctor will have have the right information to help treat it. Withholding that kind of information is probably not a good idea for your health or the health of your baby.